The following text was extracted from the lecture by Dr Michael Eades given at the 2015 LCHF convention in Cape town, S Africa.
When you put people on an intention to treat analysis, let’s say you’ve got a drug that you want to study and you put 100 people on the drug and you put 100 people on the placebo. You want to find out what the end result is overall and if a bunch of people fall out on the drug arm, you want to know that and it’ll be reflected in the statistics, because maybe they had bad side-effects. You’re trying to figure out if this drug is a marketable drug.
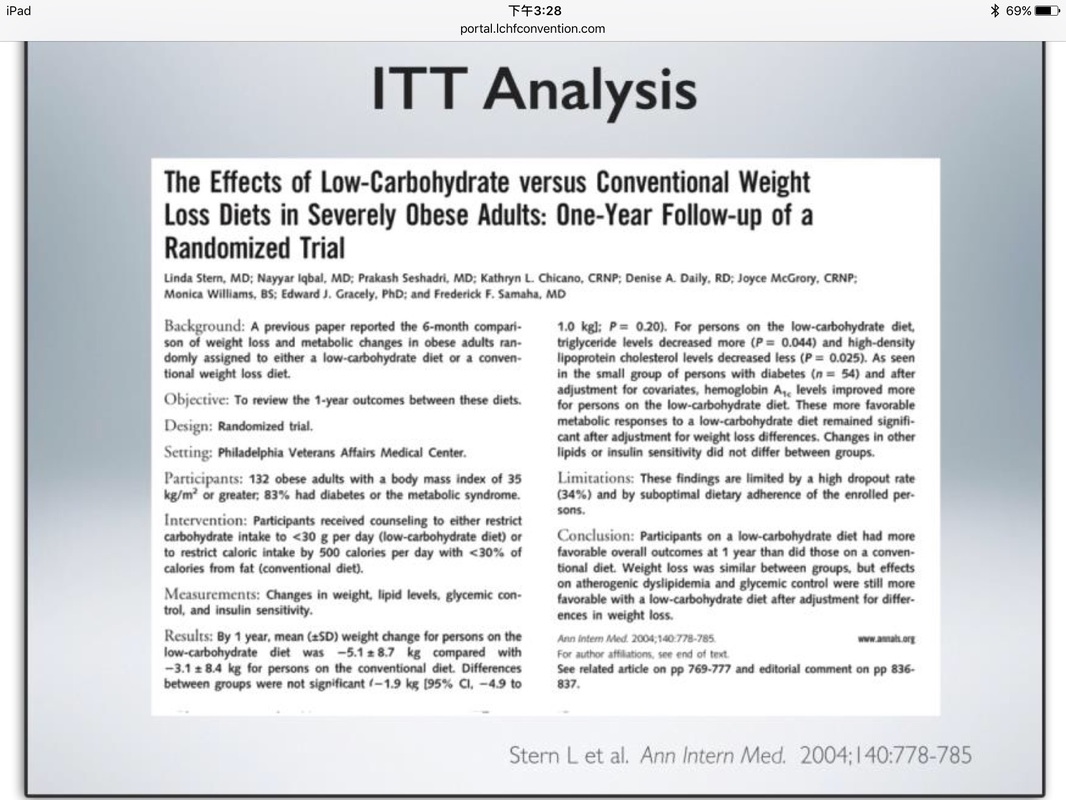
And when you do Intention to treat analysis with dietary studies, it’s terrible because here’s what happens, let’s look at two diets. You’ve diet A and diet B. Because intention to treat analysis means that everybody that goes on the study gets counted as having completed the study, whether they did or not. All right? And here you look at diet A and diet B, subjects starting study, 50 in each one, let’s say, 20 subjects completing on diet A and all 50 completed diet B. The total weight loss of people who completed the study is 60 pounds per week in each case and, so if you look at the average weight loss for your completers, you’ve got three pounds per week in diet A and you’ve got 1.2 pounds per week in diet B, so a big difference.
But if you look at it overall, if you take the people that dropped out of the diet, look at A arm of the study, everybody lost 1.2 pounds a week, so they say hey, these two diets are equal by intention to treat analysis and that’s not true. What it tells you is that diet A is a little tougher to stick on, but if you stick on it, you’re going to do a lot better and that’s the information you should be getting on this. People should say look, I’ve got two diets for you. I’ve got diet A that’s tough to follow, but if you can hang in there, you’re going to lose weight like crazy. I’ve got diet B, you go on that, it’s kind of easy, you’ll lose a little bit of weight, but that’s it, but that’s intention to treat analysis and all of these studies, they’ve used intention to treat analyses on them.
When you put people on an intention to treat analysis, let’s say you’ve got a drug that you want to study and you put 100 people on the drug and you put 100 people on the placebo. You want to find out what the end result is overall and if a bunch of people fall out on the drug arm, you want to know that and it’ll be reflected in the statistics, because maybe they had bad side-effects. You’re trying to figure out if this drug is a marketable drug.
And when you do Intention to treat analysis with dietary studies, it’s terrible because here’s what happens, let’s look at two diets. You’ve diet A and diet B. Because intention to treat analysis means that everybody that goes on the study gets counted as having completed the study, whether they did or not. All right? And here you look at diet A and diet B, subjects starting study, 50 in each one, let’s say, 20 subjects completing on diet A and all 50 completed diet B. The total weight loss of people who completed the study is 60 pounds per week in each case and, so if you look at the average weight loss for your completers, you’ve got three pounds per week in diet A and you’ve got 1.2 pounds per week in diet B, so a big difference.
But if you look at it overall, if you take the people that dropped out of the diet, look at A arm of the study, everybody lost 1.2 pounds a week, so they say hey, these two diets are equal by intention to treat analysis and that’s not true. What it tells you is that diet A is a little tougher to stick on, but if you stick on it, you’re going to do a lot better and that’s the information you should be getting on this. People should say look, I’ve got two diets for you. I’ve got diet A that’s tough to follow, but if you can hang in there, you’re going to lose weight like crazy. I’ve got diet B, you go on that, it’s kind of easy, you’ll lose a little bit of weight, but that’s it, but that’s intention to treat analysis and all of these studies, they’ve used intention to treat analyses on them.
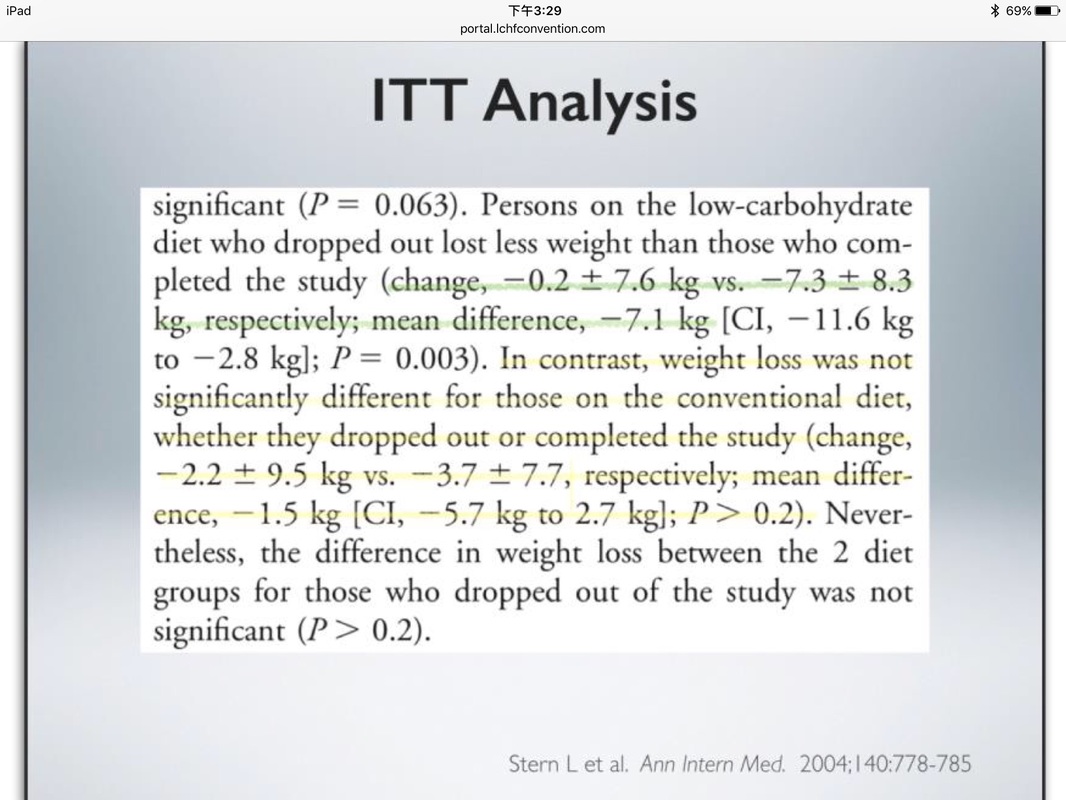
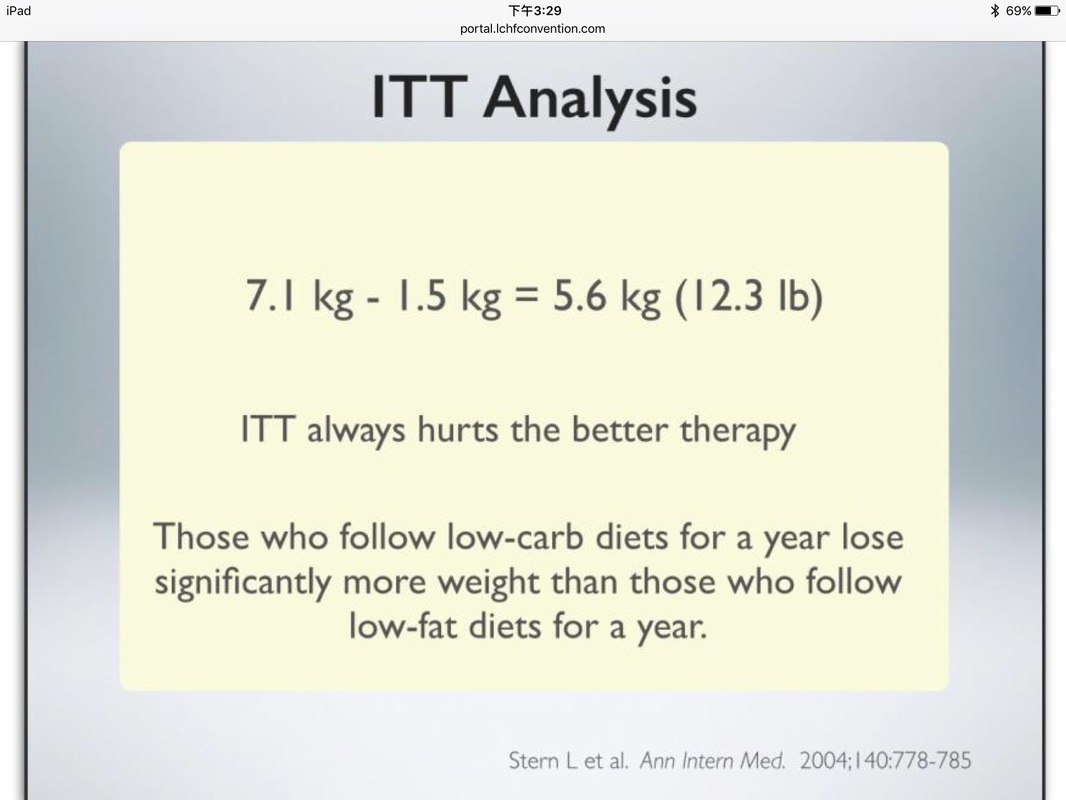
It’s always the better therapy that shows up the worst in that, so that’s why these low carb diets didn’t reach statistical significance because the people that dropped out of them, there was such a huge difference in the weight loss that the people who stayed in and the people who dropped out that it skewed the statistics, but you can't even get a study funded unless you do intention to treat analysis, so it’s tough to do.
 RSS 訂閱
RSS 訂閱
