This is incredible. It is a marker of arterial aging. The following study supports the above statement:
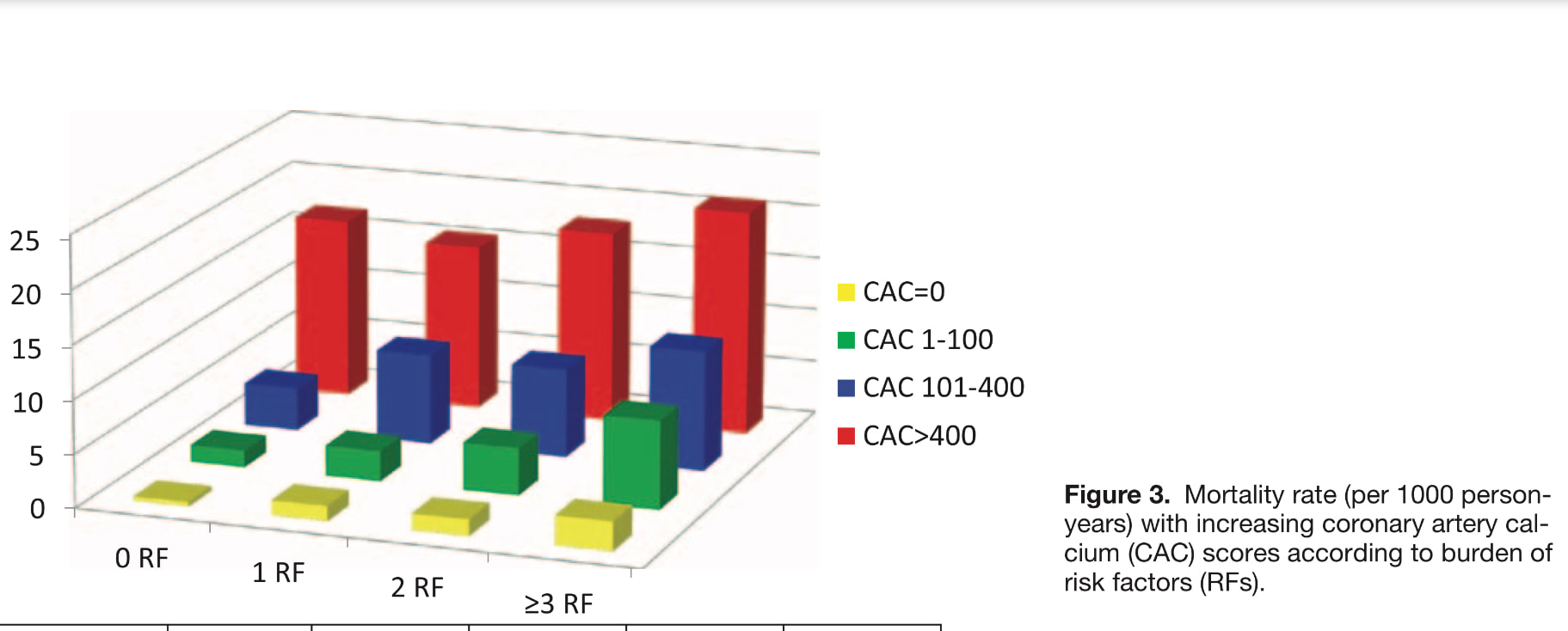
44,052 asymptomatic individuals free of known coronary heart disease underwent cardiac CT scan for the assessment of subclinical atherosclerosis (Coronary calcium score assessment). They were followed for a mean of 5.6±2.6 years for the primary end point of all-cause mortality. Individuals without traditional risk factors (smoking, dyslipidemia, DM, hypertension, & family history of coronary heart disease) but elevated CAC (who are generally not candidate for aggressive prevention) had a significantly higher mortality rates than individuals with multiple traditional risk factors but no CAC. These findings challenge the exclusive use of traditional risk assessment algorithms for determining the intensity of primary prevention therapies & suggest that selected groups of patients without traditional risk factors may benefit from further risk assessment and preventive therapies. The findings from this study are consistent with other reports: 43% of the subjects in this cohort had no traditional risk factors, & within this subgroup, 48% had detectable CAC and 6% had a CAC >400. Although prior guidelines only recommended CAC testing for select intermediate-risk individuals with 10-year risk of 10% to 20%, updated guidelines have now acknowledged the CAC testing for further risk stratification in lower risk individuals & had reduced the threshold to include individuals with estimated 6% to 10% risk of CHD in next 10 years. However, current guidelines recommend against CAC testing in those with 0 to 1 traditional risk factors. This study suggests that CAC testing even among those with no traditional risk factors provides important prognostic information, which can be instrumental in guiding preventive therapies.
44,052 asymptomatic individuals free of known coronary heart disease underwent cardiac CT scan for the assessment of subclinical atherosclerosis (Coronary calcium score assessment). They were followed for a mean of 5.6±2.6 years for the primary end point of all-cause mortality. Individuals without traditional risk factors (smoking, dyslipidemia, DM, hypertension, & family history of coronary heart disease) but elevated CAC (who are generally not candidate for aggressive prevention) had a significantly higher mortality rates than individuals with multiple traditional risk factors but no CAC. These findings challenge the exclusive use of traditional risk assessment algorithms for determining the intensity of primary prevention therapies & suggest that selected groups of patients without traditional risk factors may benefit from further risk assessment and preventive therapies. The findings from this study are consistent with other reports: 43% of the subjects in this cohort had no traditional risk factors, & within this subgroup, 48% had detectable CAC and 6% had a CAC >400. Although prior guidelines only recommended CAC testing for select intermediate-risk individuals with 10-year risk of 10% to 20%, updated guidelines have now acknowledged the CAC testing for further risk stratification in lower risk individuals & had reduced the threshold to include individuals with estimated 6% to 10% risk of CHD in next 10 years. However, current guidelines recommend against CAC testing in those with 0 to 1 traditional risk factors. This study suggests that CAC testing even among those with no traditional risk factors provides important prognostic information, which can be instrumental in guiding preventive therapies.
 RSS 訂閱
RSS 訂閱
