Dr. Salim Yusuf is the current President of the World Heart Federation. He is a world-renowned cardiologist and epidemiologist. He is also the Marion W. Burke Chair in Cardiovascular Disease at McMaster University Medical School. In Jan 2017, Dr. Yusuf publicly denounced the current dogma regarding the causes of cardiovascular disease in an effort to inspire change in the guideline treatment of this most prevalent illness. (To watch, Click Here). This video was available on youtube for a few days, then disappeared due to copyright issues. I found it on unlearn-rethink.com website, so copied the link from that website which is a good source of info about diet & health.
President of World Heart Federation talks on nutrition science -- Nina Teicholz got it right !25/2/2017
0 評論
Meal containing 60%Carb may cause higher evening postprandial insulin spike than 30%Carb meal25/2/2017 A study published in Plos one in 2016 tried to find out whether carb content matters in regard to postprandial insulin response in the evening. It is unclear whether the rise in Type 2DM incidence from 4.4 million or 2.4% of the US population in 1970s to 29.1 million or 9.3% of the population in 2014 may have been facilitated by a 30.5% increase in daily carbohydrate consumption from 213 g per day in 1965 to 278 g per day or 51% of daily calories in 2011. The currently high carbohydrate consumption falls within the 45 to 65% of daily calorie range recommended in 2010 by Departments of Agriculture and Health and Human Services. This study explores the extent to which the recommended high daily carbohydrate intake contributes to evening postprandial glucose intolerance. Postprandial hyperglycemia and delayed or protracted hyperinsulinemia are prevalent in metabolically healthy individuals in the evening but not in the morning when the same carbohydrate load is delivered as oral glucose, a carbohydrate-containing meal, or as intravenous glucose injection. Insulin hypoglycemic action for the same carbohydrate load also is lower in the evening than in the morning as shown by the requirement for a higher evening dose of insulin secretagogue tolbutamide and of insulin in type 1 diabetics. A circadian influence was recently implicated in the reduced β cell capacity to secrete insulin in the evening. However, neither this study nor two others [20,21] eliminated the possibility that the evening post- prandial hyperglycemia and delayed or protracted hyperinsulinemia result from the large daily cumulative carbohydrate load.
In the above article, two studies suggest that current habitual consumption of 51%-carbohydrate diets in the US may increase fasting insulin resistance in a clinically relevant way and promote body fat accumulation by reducing lipolysis and fat oxidation through stimulation by the high post- prandial insulin concentrations of the adipose tissue lipoprotein lipase. This study using acute one-day alteration of dietary carbohydrate content and the two studies extending it to between 5 and 14 days suggest that a reduction of carbohydrate content of the meals from about 60% to about 30% of daily energy may substantially reduce this potential risk. The answer is of course "no". However, obese persons are more likely to be insulin-resistant which means pre-diabetic. The following paper by Reaven (Diabetes Vasc Dis Res 2005;2:105-12) discusses this issue. What determines whether or not an obese person is at increased risk for CVD? The more over- weight/obese the person, the more likely they are to be insulin-resistant and at increased risk of cardiovascular disease, but substantial numbers of overweight/obese individuals remain insulin-sensitive, and not all insulin- resistant persons are obese. The results in figure 4 compare daylong glucose, insulin and free fatty acid (FFA) concentrations in response to breakfast and lunch in 20 Insulin Resistant (IR) and 18 Insulin Sensitive (IS) obese individuals, matched for age, gender, BMI and WC (Waist Circumference). The most striking difference between IR & IS persons (both are equally obese) is the post-meal insulin spikes which represents the body's attempt to push the glucose into the cells that are resistant to insulin action. 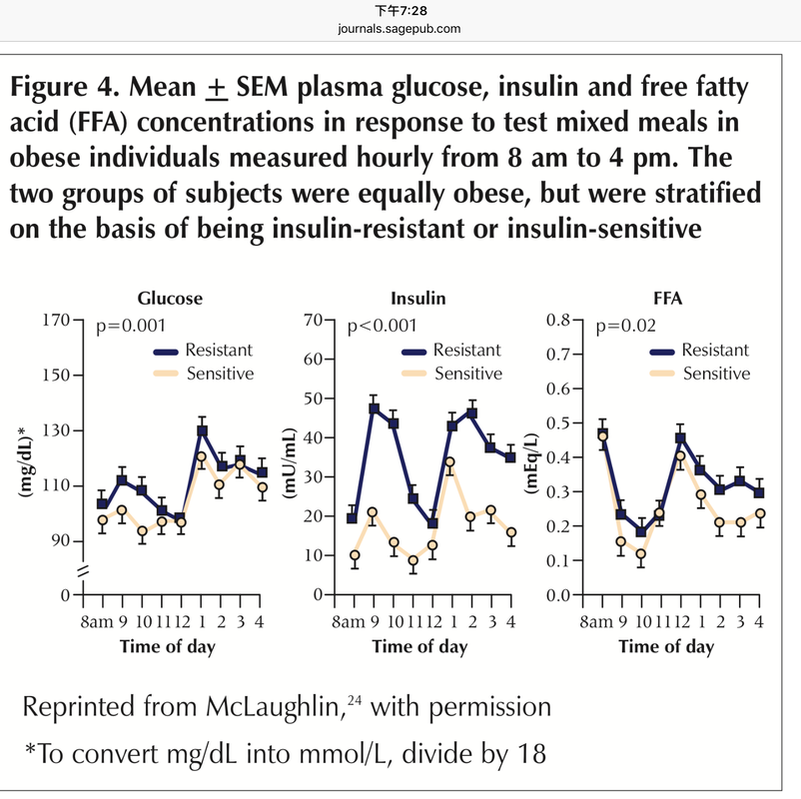 In addition to having daylong increases in plasma glucose, insulin and FFA concentrations, the C-reactive protein concentrations were also significantly higher in the IR subjects (0.39+0.08 vs. 0.12+0.03 mg/dL, p<0.005). This indicates IR subjects are more inflamed than IS persons. Inflammation is now regarded as a major contributor to CVD development.
Another issue Reaven pointed out is that measurements of BMI and WC (waist circumference) are very closely related, associated with IR to an identical degree, and CVD risk is increased primarily in those overweight/obese individuals who are also insulin-resistant. These conclusions are obviously at odds with the conventional wisdom that overweight/obesity is synonymous with insulin resistance, and the notion, codified by the ATP III and the IDF that abdominal obesity is the source of all metabolic evil. From this study, I gained one insight which could be useful in clinical practice. According to Kraft, 2 hr post-glucose plasma insulin level >40mU/ml means insulin reistance/hyperinsulinemia and also prediabetic. In fig 4 of Reaven's paper, breakfast & lunch were provided at 8:00am & 12:00 noon respectively. 1 hr & even 2 hr post-meal plasma insulin levels exceeded 40 mU/mL both after breakfast & after dinner in insulin resistant obese persons (determined by mean SSPG of 227mg/dL). In contrast, insulin sensitive obese persons (determined by mean SSPG of 76 mg/dL) have post-meal plasma insulin levels below 40 mU/mL both after breakfast & after dinner. We can check 1 or 2 hr post-meal plasma insulin level in obese persons to see whether they are pre-diabetic or not. According to Kraft, many pre-diabetics (DM in situ as Kraft called them) that could be missed by standard OGTT can be detected by OGTT plus plasma insulin assay. However, giving patients 100g glucose load and checking insulin 2 hrs later is hard to perform in practice. This study provides evidence that post-meal insulin could be more practicable & pick up those who are at increased risk of CVD.      Boil tomato a few minutes, cut into 4 pieces & remove the skin. Use a blender to make tomato juice & pour it over the base. Add 50g chopped sausage (cooked), 35g precooked mushroom, 35g precooked green pepper, 50g mozzarella cheese on top. Bake at 175C for 5 minutes.
番茄水煮一下,用刀切十字型,把皮剝掉,番茄肉用果汁機打成汁然後澆在披薩底上。把50克的香腸(煮熟切小塊),先炒過的蘑菇35克,先炒過的青椒35克,(莫扎里拉)起司50克灑在底部上,用175度C考5分鐘 Pizza 就完成了。 |
Archives
七月 2021
Categories |
 RSS 訂閱
RSS 訂閱
